
In the past we have talked about frostbite and other types of cold weather. One thing we haven’t talked about is cold weather trauma. Things work different in the cold. One of the biggest things medics do is strip down a patient to be able to see any injuries.
The problem with that is that we expose the patient to further cold injury. This means a old but new to some technique for evaluating or patients.
This tip of the week is cold weather triage
Lets talk a bit about the steps in triage
Patient Assessment. This starts at some basics and we need to modify them for OUR use.
First of Scene Size Up. When we arrive we look and see first where the patient is. Then we look for hazards at the scene. Wild animals, thin ice, armed insurrection storm debris what ever. It is important to make sure YOU the medic is reasonably safe. You do no one any one if you are hurt or worse.
MOI or Method of Injury. Blast damage, penetration, trauma, cuts, falls. Each one takes an different approach. Hazards are covered at the beginning. Remember to keep your eyes and ears open.
BSI. Body Substance Isolation. The icky part.30 years ago a medic tech or nurse was considered, “a wuss” if he treated a person with gloves. Today I look back on those says with amazement that I an not sick or worse after being “elbow deep” In someone’s chest. Today it is standard precautions. In reality the skin with no breaks cuts or abrasions is a better barrier to bugs than anything else. BUT the waterproofing goes away in a mater of hours in constant immersion.
ABC‘s. In all reality the ABC’s have been of 2 forms Airway, Breathing and Circulation. Or Airway Breathing and Compressions We are concerned with the circulation part. Those are pretty self explanatory.
When we move on to Environmental Exposure. Here we get to the meat of the topic for this week.
This is where we decide if we treat on site or move. A few things come up with this. First CAN you move. Should you move.
Lets focus the tip of the week here. How to examine triage and determine if a person or how much they are hurt. First is un witnessed as What Happened? While the patient is telling you what happened observe the patient’s body language. Look and listen to what they are saying how they are saying
Next while they are CLOTHED ask Where does it hurt? Old EMT method we would start striping the patient and doing a visual as well as physical exam. In the temperatures listed above that is an invitation for disaster.
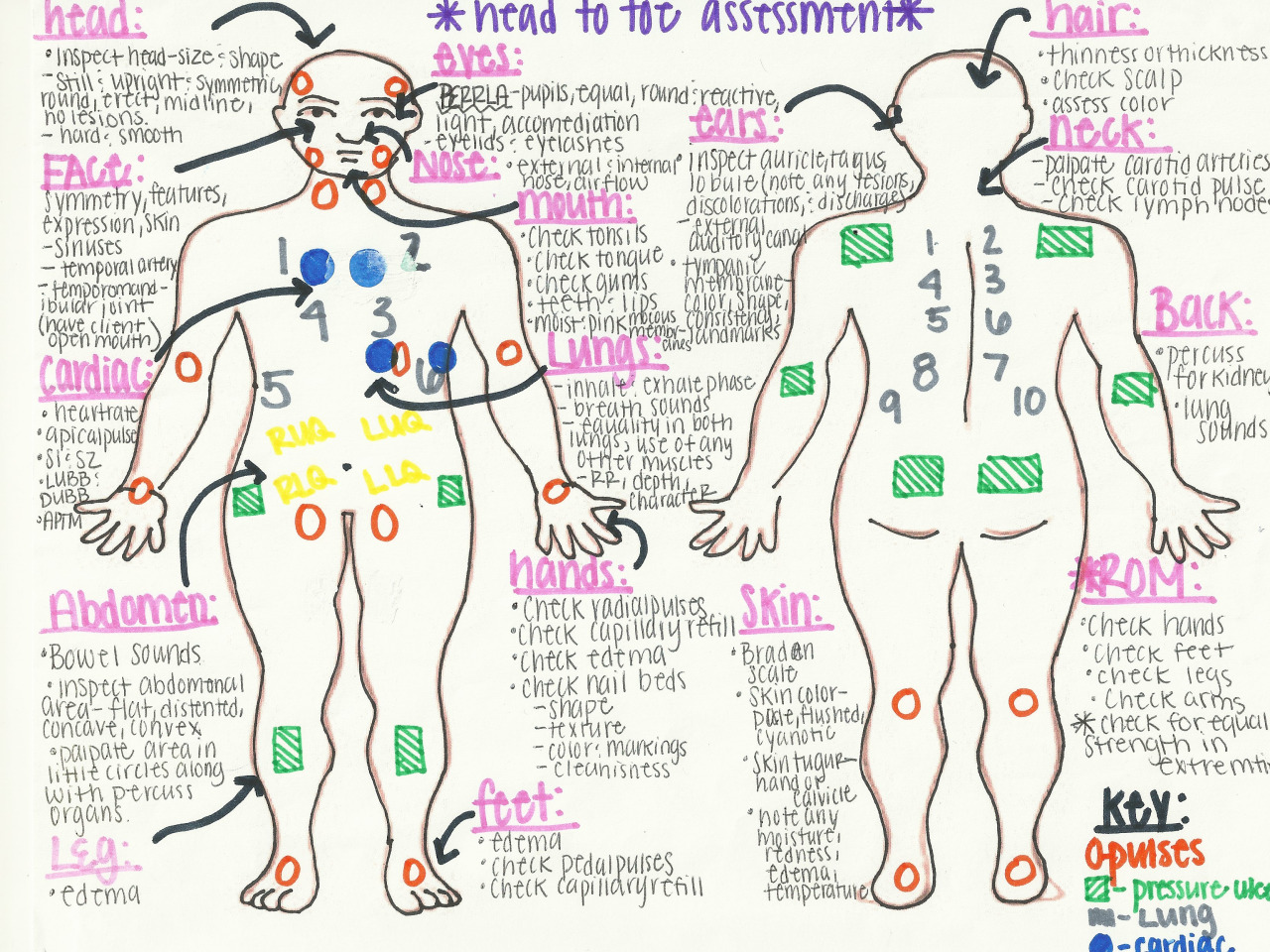
Head to Toe Assessments That is in progress
Vital Signs. This is where we do a quick set of vitals Pulse rate And respiration. BP at this point is not indicated to be taken UNLESS the patient is unresponsive.
Here we ask Where does it hurt. And deviate from the standard of expose the injuries. Here we would feel and look to see .
Also we can determine if he is Disorientated. IE Where does it hurt? And he answers, Tuesday. Lets assume he is orientated to time/date place and name (In the TV shows you’ll hear “He is orientated times 3” Thats what it means) Also CSM is evaluated (Circulation / Sensory / Motor) We look at the finger tips, fingers and hands and toes feet and ankles. and check for color movement and sensations. Just unlace the boots don’t remove them. And we ask for allergies, and don’t forget food allergies.
Medications. This is so important. Medications can effect so much of what is going on with a patient. Also don’t forget the herbal medication.
Decision on Disability. This doesn’t mean the social security type on decision. It means that you need to decide if you need to implement and or continue cervical spine precautions.
SCTM or Skin Color, Temperature, and Moisture. This is how we help determine if the circulation is work and if the patient is going into shock Or hypothermic
Lastly it is Last in Last out. When was the last time you had anything to eat or drink the last time you urinated and had a bowel movement. And where they normal for YOU. Odd but needed. The first assess if we have to worry about vomiting, the next tells us that prior to the fall he had blood in his stool or urine OR didn’t and we will watch to see if he develops any.
Cold weather triage is a bit more different than warm weather. You can’t just whip out the shears and start cutting away clothing and jackets. Now in the current time we are in we actually have patterns for cutting clothes away so that they can be put back to help keep the patient warm, but they are useless for wear anymore until a GOOD person with a sewing machine gets to them. In a survival situation and if the patient is going to survive you need to think ahead and triage with out cutting off the clothing. A lot of the things we take for granted are not going to be there.
All of this plays into caring for trauma. First you can use the cold to help control bleeding, Also it has a mild anesthetic effect. But also it can cause a lot more harm.
The key to this is to:
**KEEP THE PATIENT WARM**
1.Protect the patient from further injury due to the cold.
2. Do a complete and detailed exam. Do not miss anything.
3 All the while, be thinking of getting your patient OUT of the elements.
4. While examining, expose what is needed and then cover
5. Involve the patient
6 And did I mention KEEP THE PATIENT WARM?
We’ll leave it here for now. Next week we’ll talk about cold weather orthopedics INCLUDING how to clear a patients C Spine with out Xray
Sign up for our news letter and get the FULL tip of the week.